Skin perfusion pressure — SPP
SPP is a noninvasive method that leverages laser Doppler to measure blood perfusion in the microcirculation. It is primarily used in clinical (and clinical research) settings to assess wound healing potential — especially in patients with chronic conditions such as diabetic foot [1].
One of the main advantages of SPP is that it is not affected by vascular calcification or anatomical structure. When clinical conditions — such as wounds on the sole or amputated toes — preclude the application of toe pressure or TcpO2, SPP is a viable alternative.

SPP with PeriFlux 6000
It’s possible to carry out toe pressure and SPP in a single patient visit.
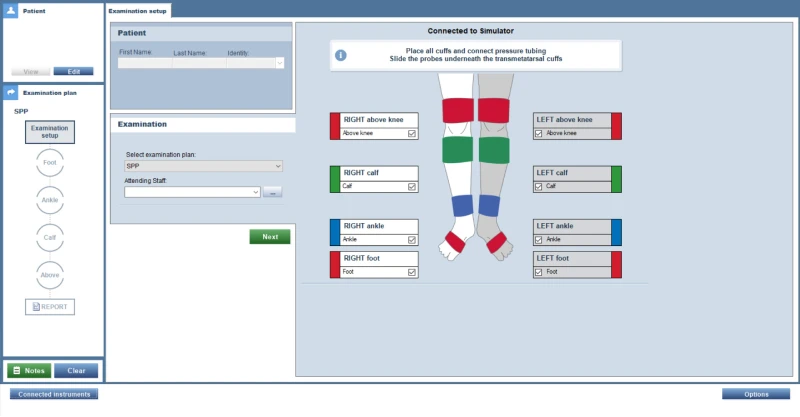
SPP can be measured at multiple sites: on the foot (plantar, dorsal, and toes), on the ankle, and above and below the knee. Blood flow is occluded by placing a pressure cuff over the probe and inflating it above the patient’s resting systolic pressure. The cuff is then gradually deflated until microcirculatory flow returns — this is the SPP value and is measured in millimeters of mercury (mmHg).
SPP can help identify ischemic areas (by, for example, using the angiosome concept). Comparing SPP measurements in areas adjacent to a non-healing ulcer can reveal microcirculatory vascular deficiencies.
How to carry out SPP with PeriFlux 6000
When to use SPP
Not all patients are the same, toe pressure, for example, isn’t feasible for a person whose toes have been amputated. For patients with edema, callouses, or wounds on the sole or plantar region, SPP is the most applicable means for measuring the microcirculation.
Interpreting SPP results
The 2023 update of the IWGDF guidelines [2], includes SPP values for wound-healing prognosis, stating that values ≥ 40 mmHg can increase the probability of healing by up to 30%.
Download our eBook
The main advantage of SPP is that it is not affected by vascular calcification and anatomical structure. [3]
Related products and applications





Contact us
Get in touch
If you would like to know more about how to use skin perfusion pressure, its application, or our related products, fill out the form and we will be in touch with you shortly.
References
- Gornik, H. L., Aronow, H. D., Goodney, P. P., Arya, S., Brewster, L. P., Byrd, L., Chandra, V., Drachman, D. E., Eaves, J. M., Ehrman, J. K., Evans, J. N., Getchius, T. S. D., Gutiérrez, J. A., Hawkins, B. M., Hess, C. N., Ho, K. J., Jones, W. S., Kim, E. S. H., Kinlay, S., Kirksey, L., … Wilkins, L. R. (2024). 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS Guideline for the Management of Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation, 149(24), e1313–e1410. https://doi.org/10.1161/CIR.0000000000001251
- International Working Group on the Diabetic Foot (IWGDF). Guidelines on the prevention and management of diabetic foot disease (2023 update). https://iwgdfguidelines.org
- Pan, X., Chen, G., Wu, P., Han, C., & Ho, J.K. (2018). Skin perfusion pressure as a predictor of ischemic wound healing potential (Review). Biomedical Reports, 8, 330-334. https://doi.org/10.3892/br.2018.1064