Clinical research
Built on advanced signal processing and laser Doppler technology, our solutions provide comprehensive insights into macro- and microcirculation. They can be used in a range of clinical research applications, including dermatology, endothelial dysfunction, and exercise physiology. Our technologies are designed to facilitate data collection and generate robust insights that help clinical researchers deliver data-driven findings.

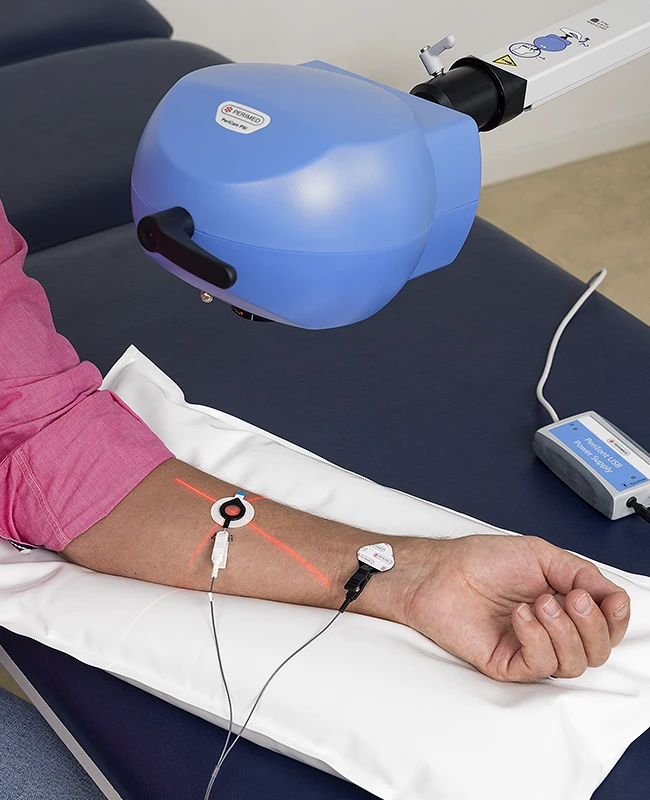
Iontophoresis
Iontophoresis is a useful clinical research method that provides a noninvasive means to deliver certain types of drugs directly through the skin.
The process is easy to carry out, it supports precise, localized delivery, and is painless for the study participant.
Combining laser speckle measurement with iontophoresis enables researchers to assess the impact of drugs and novel compounds on the microcirculation in real-time.

Post-occlusive reactive hyperemia (PORH)
PORH is a noninvasive method used to investigate and assess microvascular function. The exam involves taking blood perfusion measurements before, during, and after a prolonged occlusion.
To avoid undue patient discomfort, pressure exams involving occlusion typically last up to about one minute in clinical settings. In a PORH exam, however, the typical occlusion time is around 5 minutes. After the pressure in the cuff is released, the hyperemic response is measured, which reflects vascular reactivity and the capacity of the blood vessels to dilate and restore perfusion. The recovery phase is often monitored for several minutes.
In clinical research, PORH could be used to:
- Evaluate microvascular function — identify early signs of endothelial dysfunction, a precursor to conditions like atherosclerosis.
- Therapy efficacy — monitor how treatment impacts vascular reactivity.
- Predicting disease progression: — understanding the role of impaired reactivity in vascular diseases like PAD.
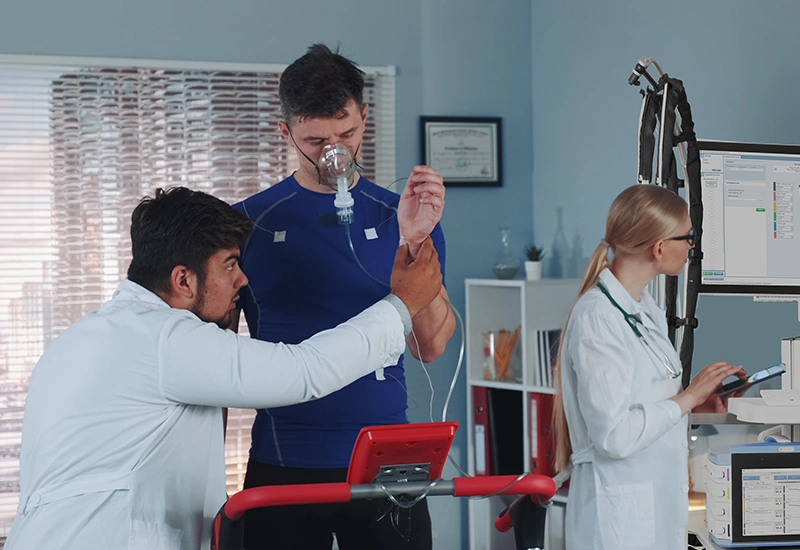
Exercise physiology
Laser Doppler flowmetry (LDF) is a suitable technology for clinical research to reveal the effect of physical activity on microcirculation in the study of thermoregulation, cutaneous vasodilatation, and heat stress, for example. Healthy and diseased populations are of interest, as research can improve understanding of athletic performance and the mechanisms of vascular diseases.
Our LDF solution for clinical research includes a monitoring device with a heated laser Doppler probe. The heated probe can be used to elicit a thermoregulatory response or to maintain consistent experimental conditions. Post-occlusive reactive hyperemia (PORH) can also be used together with LDF in exercise physiology.
Read more about our clinical research product PerifFlux 6000 Laser Doppler Perfusion Montitoring.
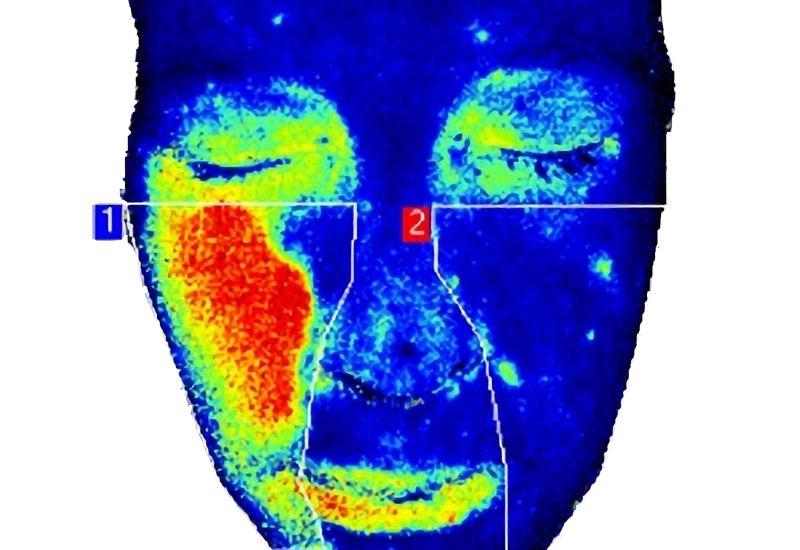
Dermatology
Laser speckle contrast imaging (LSCI) is useful in clinical research because it is a noninvasive technology for real-time assessment of skin conditions such as inflammation, wound healing, and vascular changes.
Without the need for contrast agents, LSCI preserves tissue integrity, supporting accurate microvascular analysis. By leveraging LSCI, our PeriCam PSI instruments can deliver robust data to validate treatment efficacy and underpin findings.
Read more about the versatility of PeriCam PSI NR.
Endothelial dysfunction
Endothelial function is a tissue impairment in people with diabetes, especially via reduced NO production. This pathological state can contribute to diabetic complications, and as such is a potential target for the prevention of complications related to diabetes[1].
An increasing amount of evidence links endothelial dysfunction to cardiovascular outcomes such as stroke, heart attacks, or risk for the development of diabetes[1]. Endothelial function can be studied by performing tests that cause endothelium-dependent or independent vasodilation, such as post-occlusive reactive hyperemia (PORH), thermal challenge with laser Doppler flowmetry, and iontophoresis.
Related products




Contact us
Get in touch
For more information about using our products in clinical research, fill out the form and we’ll get back to you shortly.
References
- Takeda, Y., Matoba, K., Sekiguchi, K., Nagai, Y., Yokota, T., Utsunomiya, K., & Nishimura, R. (2020). Endothelial Dysfunction in Diabetes. Biomedicines, 8(7), 182. https://doi.org/10.3390/biomedicines8070182
LASCA and LSCI
Laser speckle contrast imaging (LSCI) is the innovative technology behind PeriCam PSI, offering non-contact, high-resolution perfusion imaging. The technique was first described by J.D. Briers and S. Webster in 1996 and referred to as laser speckle contrast analysis (LASCA). In later years, the term LSCI gained in popularity and is nowadays the more common term. However, LSCI and LASCA both refer to the same technique, providing precise and reliable perfusion data without the need for contrast agents.