
Filling the technology gap in oncoplastic surgery — with perfusion imaging

In his upcoming paper on the use of laser speckle contrast imaging (LSCI) in oncoplastic reconstructive breast surgery, Dr. Damian Ralser of the University Hospital of Bonn in Germany concludes that the technology holds considerable potential for intraoperative decision-making. Ralser and his colleagues conducted an observational study on 54 patients (73 reconstructions); their findings suggest that surgeons can leverage the rapid insights from LSCI to reduce complication rates, particularly perfusion-related complications such as tissue death (necrosis).
In this post, I will outline some of Dr. Ralser’s findings together with a few of my thoughts on the use of LSCI in plastic surgery.
Time is tissue
According to the American Cancer Society [1], breast cancer accounts for almost one-third of female cancer patients in the US. One study [2], states that nearly 30% of all implant procedures result in a complication, with almost half classified as major. In addition to potentially compromised oncological outcomes, failed reconstruction can have significant physical, emotional, and financial consequences for patients.
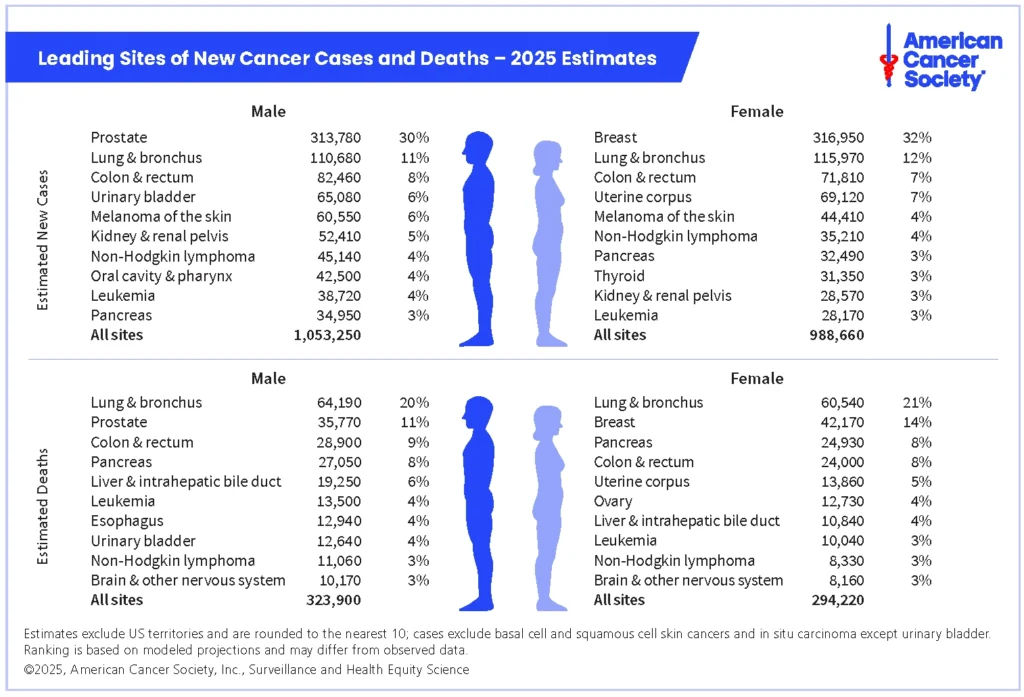
American Cancer Society. Cancer Facts & Figures 2025. Atlanta: American Cancer Society; 2025.
Finding a solution is rarely easy; technologies need to be tested clinically, which means time and some pre-indication of success to secure the necessary funding and buy-in. Ralser and his team have found potential in LSCI.
Skin perfusion is a powerful early indicator of necrosis because it directly reflects how well blood — with its healing oxygen and nutrients — is delivered to tissue. Lack of adequate perfusion is often the root cause of necrosis. When blood flow is low, skin cells don’t receive the oxygen and nutrients they need, leading to hypoxia, cellular damage, and eventually cell death.
By the time necrosis is visible, it’s usually too late to reverse. Measuring skin perfusion helps surgeons detect early signs of compromised blood flow, allowing for intervention that can prevent tissue loss. But measuring perfusion can be challenging, especially during surgery.
The measurement challenge
According to Ralser,
“…the clinical subjective assessment of skin perfusion by the surgeon based on skin color, temperature, dermal bleeding, and in particular clinical experience, remains the primary method for evaluating tissue perfusion intraoperatively.”
Indocyanine green (ICG) angiography offers an alternative method for assessing skin perfusion during a procedure. This method requires the injection of a fluorescent dye that binds to proteins and plasma. Because the dye remains within the blood vessels, it is a viable solution for perfusion assessment. Under near-infrared light, the dye fluoresces, which can be captured by a specialized camera. The intensity and pattern created by the dye, along with how quickly the dye moves through the body, provide an indication of perfusion. However, according to Ralser, it has yet to be routinely adopted in clinical care.
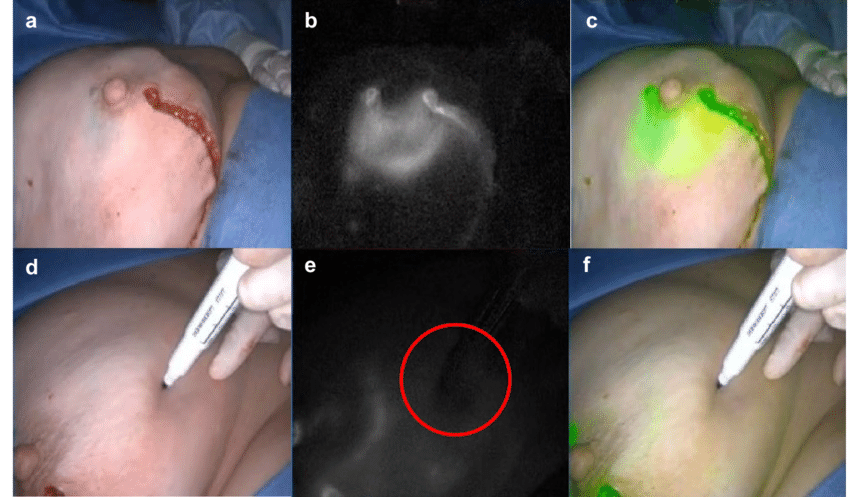
Intraoperative ICG imaging (b, e) shows reduced perfusion (circled dark region in picture e) after implant-based reconstruction following nipple-sparing mastectomy in comparison to native intraoperative images (a, d). The SPY software enabled an overlay (c, f) of ICG imaging and native pictures. The upper (a, b, c) and lower (d, e, f) row of pictures show different perspectives on the reconstructed breast
[3] Image courtesy of Kühn et. al., 2020 — no changes made
ICG is an invasive point-in-time measurement that requires multiple injections for multiple measurements. Assessment can be challenging as injured blood vessels may lead to dye leakage. Overall, complex and costly.
Why LSCI?

I’d say the main reasons clinical researchers like Ralser are looking to LSCI as an alternative method for measuring blood perfusion are its ease of use, noninvasiveness, and non-contact nature. First, you don’t need any contrast agents, which eases measurement for everyone in the operating theater. Unlike ICG, LSCI isn’t limited to short measurement windows. With an LSCI instrument like PeriCam PSI (used in Ralser’s research), you place the instrument head about 20-25cm above the measurement area and record. Without the need for direct contact with the patient’s skin, LSCI offers distinct benefits over probe-based solutions, such as ultrasound.
LSCI instruments provide an instant overview of blood perfusion in the measurement area, which you can compare with previous measurements, including pre-op levels. Ralser’s research indicates that perfusion is lowest immediately after surgery, improving in the 72 hours post-op, and is significantly reduced in patients with postoperative complications.
I’d say that this ability to deliver quantifiable data is the other major advantage of LSCI compared with traditional blood perfusion measurement techniques. The real-time visualization of perfusion helps surgeons make rapid decisions while patients are on the table, and the underlying perfusion data enables objective comparison of areas of the skin over time.
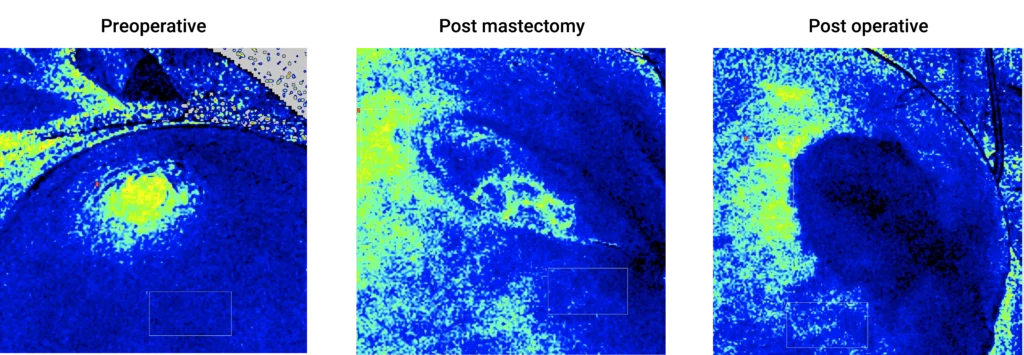
The above images, generated by PeriCam PSI NR on one of the study participants, clearly show a lack of perfusion in the nipple area, and the patient underwent subsequent surgery.
What does it mean for patients?
More research is needed before LSCI becomes fully adopted, but the preliminary indications are positive. In his study, Ralser had only one case of necrosis, which is low. According to [4], the reported failure statistics range between 2%-22%. However, even these figures may be low due to differing definitions and varying conditions of the selected patients. Ralser also notes in his study that additional research needs to be carried out on a homogeneous cohort.
If you want to watch our webinar with Dr. Ralser, where he presents these findings, you can sign up to watch it here:
If you want to know more about PeriCam PSI, the instrument Dr. Ralser used to carry out his research, you can read more about it here: PeriCam PSI NR.
I hope you found this post insightful.
Jimmy Bakker
Product Manager Imaging and Research

I’ve been with Perimed for over 10 years, and in my role as PM for our imaging solutions, I get to work with amazing people who use our instruments to improve outcomes and find novel therapies for some of the world’s most prevalent diseases. I have a Master’s degree in applied physics and a Ph.D. in applied optics.
References
- American Cancer Society. Cancer Facts & Figures 2025. Atlanta: American Cancer Society; 2025. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2025/2025-cancer-facts-and-figures-acs.pdf
- Bucher, F., & Vogt, P. M. (2022). The Failed Breast Implant in Postmastectomy Reconstruction: A Systematic Literature Review of Complications of Implant-Based Breast Reconstruction. Annals of plastic surgery, 88(6), 695–703. https://doi.org/10.1097/SAP.0000000000002980
- Kühn, F., Blohmer, J. U., & Karsten, M. M. (2020). Intraoperative indocyanine green fluorescence imaging in breast surgery. Archives of gynecology and obstetrics, 302(2), 463–472.
https://doi.org/10.1007/s00404-020-05582-7 - Matsen, C. B., Mehrara, B., Eaton, A., Capko, D., Berg, A., Stempel, M., Van Zee, K. J., Pusic, A., King, T. A., Cody, H. S., 3rd, Pilewskie, M., Cordeiro, P., Sclafani, L., Plitas, G., Gemignani, M. L., Disa, J., El-Tamer, M., & Morrow, M. (2016). Skin Flap Necrosis After Mastectomy With Reconstruction: A Prospective Study. Annals of surgical oncology, 23(1), 257–264.
https://doi.org/10.1245/s10434-015-4709-7
Disclaimer
The views and opinions expressed in this blog post are solely those of the author and do not necessarily reflect the official position or policies of Perimed. The content provided here is intended for informational purposes only and should not be interpreted as clinical claims or medical advice. Readers should consult healthcare professionals for specific medical concerns or treatment options.